With other payers looking at Medicare’s actions on telehealth coverage, a Kaiser Family Foundation brief offers insights on Medicare beneficiaries that support the permanent expansion of connected health services.
– Medicare beneficiaries are using telehealth more often due to extended coverage and access measures introduced during the COVID-19 pandemic, according to a Kaiser Family Foundation brief. And making these measures permanent could further benefit members and influence other payers to follow the same strategy.
Prior to the pandemic, Medicare only covered telehealth services for members living in rural areas, with restrictions on where members could receive services and which providers could deliver them. The Centers for Medicare and Medicaid Services expanded coverage in early 2020 to address the pandemic, and renewed the extension in April 2021, to allow members to access healthcare services while avoiding in-person contact.
For its study, KFF collected telehealth use data from Medicare beneficiaries between summer and fall of 2020. Kaiser researchers noted the increase in use among members, as well as the populations who used telehealth more frequently during the COVID-19 emergency.
Of the Medicare members with an established source of care, almost two-thirds (64 percent) reported that their provider offered telehealth appointments. Before the pandemic, only 18 percent of members could say that. Some beneficiaries reported that they did not know if their provider offered telehealth services, including almost one-third (30 percent) of members living in rural areas.
More than a quarter (27 percent) of Medicare and Medicare Advantage beneficiaries had a telehealth visit with a healthcare professional, according to the survey, which equals 15 million people who used telehealth during the pandemic. Of the members whose established providers offered telehealth, almost half (45 percent) had a telehealth visit.
Telehealth use was higher among beneficiaries under 65 who qualify for Medicare due to a long-term disability, dual eligible beneficiaries, Black and Hispanic beneficiaries, and beneficiaries with six or more chronic conditions, with more than 50 percent of each group reporting using telehealth.
The study also offered evidence supporting continued coverage for audio-only telehealth services, which have been popular during the pandemic.
More than half (56 percent) of Medicare beneficiaries who used telehealth reported using a telephone for their visit. Of those, 65 percent were 75 or older, 61 percent were Hispanic, 65 percent lived in rural areas and 67 percent were dual eligible enrollees.
Audio-only telephone visits are permitted during the public health emergency but will be dropped from coverage once the PHE ends. KFF research indicates that permanent coverage of audio-only telehealth could benefit older beneficiaries, people of color and, beneficiaries living in rural areas, especially since less than half of Black and Hispanic beneficiaries (42 and 34 percent) own a computer.
Under Medicare’s emergency extensions of telehealth coverage, healthcare professionals can provide and get reimbursement for telehealth services; prior to the pandemic, that coverage was limited to telehealth services for patients who’ve been meeting with the provider for at least three years.
CMS has also extended telehealth services to rural health clinics and federally qualified health centers, locations not covered under pre-COVID-19 rules.
CMS has increased telehealth reimbursement rates during the pandemic as well, in some cases offering payment parity – a factor that, if extended, could pull more providers onto the platform. Reimbursement has long been a challenge to telehealth adoption, with providers saying they aren’t being paid enough to try new platforms and payers arguing that they should be able to negotiate their own rates with care providers.
Medicare Advantage plans are more telehealth-friendly, with 98 percent covering connected health services to members even before the pandemic.
Still, the path to increased or even permanent coverage is uneven.
In May 2021, the Government Accountability Office told Congress to hold off on expanding Medicare telehealth coverage past the public health emergency, citing concerns about spending, program integrity, patient health and safety, and equity. The GAO is asking for more evidence showing that telehealth services are cost-effective and produce positive health outcomes for Medicare beneficiaries.
The results from the KFF brief show the impact that expanded telehealth coverage has had on members and how these outcomes could help influence Medicare and other payers’ decisions about telehealth coverage going forward.
Schools and Libraries Will Have 45 Days to Apply for Support to Aid Students Who Fall into the Homework Gap
WASHINGTON, June 15, 2021—Today, FCC Acting Chairwoman Jessica Rosenworcel announced schools and libraries can begin to file applications on June 29 for the newly established $7.17 billion Emergency Connectivity Fund. Schools and libraries can apply for financial support to purchase laptops and tablets, Wi-Fi hotspots, modems, routers, and broadband connections for off-campus use by students, school staff, and library patrons. During this 45-day application filing window, which will run from June 29 to August 13, eligible schools and libraries can submit requests for funding to purchase eligible equipment and services for the 2021-22 school year.
“For too long, the Homework Gap has been a troubling and persistent digital equity problem in the United States,” said Rosenworcel. “With classes themselves moving online and the pandemic requiring us to stay home, we went from having millions of children who couldn’t do online homework assignments to having millions of children who couldn’t do schoolwork at all. In other words, the Homework Gap became a full-fledged learning and education gap.”
“It’s important that we address this issue now, and the Emergency Connectivity Fund gives us the opportunity to do that. As we exit this pandemic, we know that education has been changed. Like so much else in our lives, it has been digitized. That’s why I’m proud that starting in two weeks, schools and libraries across the country will have a terrific opportunity to get broadband service and devices into the hands of students, staff, and library patrons who lack them to connect these learners at home,” said Rosenworcel.
The American Rescue Plan of 2021 established the Emergency Connectivity Fund. The Universal Service Administrative Company will serve as the program’s administrator with FCC oversight. The Fund leverages the processes and structures used in the E-Rate program for the benefit of schools and libraries already familiar with the E-Rate program. You can find more information about the program at www.emergencyconnectivityfund.org or www.fcc.gov/emergency-connectivity-fund and instructions on how to apply at www.emergencyconnectivityfund.org/application-process.Recent estimates suggest there may be as many as 17 million children struggling without the broadband access they need for remote learning. Since her early tenure at the Commission, the Acting Chairwoman has made closing the Homework Gap a priority.
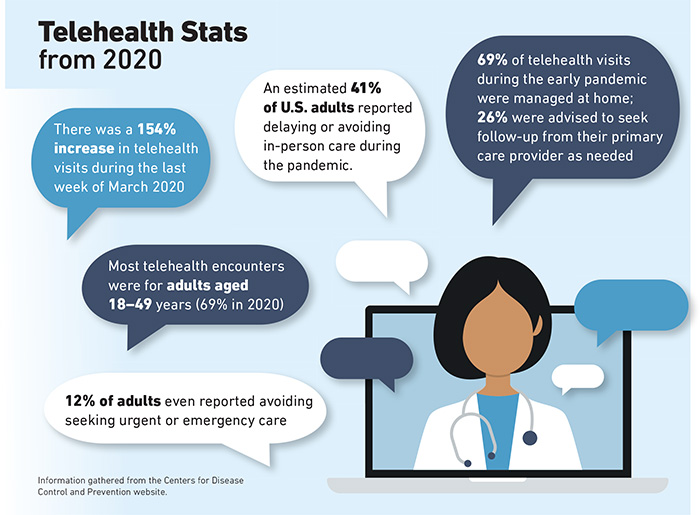
At the height of the COVID-19 pandemic, people were working at home, teaching their children at their kitchen tables, and avoiding various activities including in-person visits with their doctors.
As a result, for a few months at the start of the pandemic, the use of telehealth and telemedicine exploded.
The Centers for Disease Control and Prevention reported that telehealth visits were up 154% in the last week of March 2020, compared to the same period in 2019.
Today, as more people in the U.S. become vaccinated, it appears that spike in telemedicine use has flattened, but some questions linger: Is interest in telehealth here to stay and will it play a major role in cost containment and service delivery in workers’ compensation?
Statistics support the notion that there is increased acceptance of telehealth. According to McKinsey, 46% of patients say they now use telehealth for some visits, compared to 11% in 2019.
Melissa Burke, vice president, AmTrust Financial Services, Inc.
An increase in telehealth caused by the pandemic was witnessed by David Lupinsky, vice president of digital health and innovation at CorVel.
He said his company reported more telehealth visits in the last two weeks of March 2020 than they had in the previous two years combined.
“It had been going up [in the previous two years], but we saw a huge spike of nearly 500% in March 2020,” he said.
That number has dropped, though it hasn’t gone down to pre-pandemic levels, he said.
His company receives about 100,000 calls a year to its nurse triage hotline, which is staffed by nurses who refer patients to self-care, telehealth or an in-person visit at a medical office or clinic.
About 70% of claims filed at CorVel start with a call to the nurse triage hotline. About 50% of calls are resolved with the nurse recommending self-care for patients, which results in no claim. Of the other half, about 45% are referred to telehealth and 55% end up going into a physical office for a doctor’s visit.
Well-Defined Benefits
In addition to helping to mitigate the spread of disease during a pandemic, Lupinsky said telehealth has a myriad of other advantages for injured workers and employers.
“There are so many other benefits of telehealth,” he said. “There is obviously a return on investment there. It helps reduce the medical spend and improve the speed to get [a patient] to a provider.”
He noted that nurses answer the company’s triage phones within 30 seconds, and a physician will respond to a referral for a virtual telemedicine visit within 10 minutes. A movement in some states to allow doctors to be licensed across state borders also has been a boost for telehealth.
Jennifer Cogbill, vice president of the GBCare Advisor Team at claims service provider Gallagher Bassett, also saw a 15% increase in telehealth-related medical bills in the first 90 days of the pandemic.
That number has since dropped to about 2%.
Like Lupinksy, Cogbill said there are areas in workers’ compensation claims where telehealth is particularly useful, such as triaging patients to determine the type of care they need.
She said she hasn’t seen telehealth used much in workers’ compensation beyond that point-of-injury care and attributes that, in part, to a lack of investment in the technology.
“A lot of providers never invested in the ability to provide a secure connection for a telemedicine visit, although [with the pandemic], we saw providers starting to offer it,” she said.
Cogbill believes telehealth is well-suited for use in ongoing care to monitor a person’s recovery from an injury or minor illness.
“I believe there is a lot of opportunity for telemedicine in follow-up care, but that needs to be promoted by the provider community,” she said. “I think there are some who’ve made that investment and who want to continue to offer that.”
An Innovative Tool
Melissa Burke, vice president at AmTrust Financial Services, Inc., said telehealth is just one way to address patients’ needs.
“It’s another tool in our tool belt,” she said. “It’s about looking at the injury and seeing what makes sense for treating that injury.”
Her company has used national guidelines to train staff on what types of injuries are suited to telehealth.
Like Cogbill, she sees follow-up care as one area where telehealth may be especially useful. Another area is behavioral health.
“We’ve seen an increase in acceptance of telehealth and I think that’s going to continue,” Burke said.
Still another area where telehealth may prove beneficial is in physical therapy that would begin with in-person visits but evolve into virtual visits as a person’s condition improves.
Burke said the pandemic has raised awareness of telehealth, including among her company’s employees.
“Our claim and medical professionals are aware that this service is available and how it can improve the claims process,” she said.
“It can allow employees to be treated at work without having to leave the work site or transition back to work when they do things like tele PT or behavioral health.”
Terri Rhodes, chief executive officer at Disability Management Employer Coalition, agreed that the pandemic has accelerated adoption of telehealth: “In 20/20 hindsight, it wasn’t just that patients weren’t using it,” she said. “Doctors weren’t using it either. So, I think we were all forced into it, and very quickly we had to figure it out.”
Other forces boosting telehealth during the pandemic included the federal government, state Medicaid programs and private insurers that expanded coverage for virtual health care services during the crisis.
The U.S. Department of Labor also allowed telemedicine in lieu of in-person treatments under the Family Medical Leave Act.
Looking Ahead
While experts agree that telehealth is useful in some workers’ compensation situations, it still has shortcomings.
Rhodes said a potential disadvantage is that “a medical professional might miss minor signs or symptoms resulting in an inaccurate or incomplete diagnosis, because you really can’t see that person. You can only see what they’re showing you on camera.”
Technology, of course, with its problems of faulty internet connections or dropped calls, can be a deterrent, and some employers are reluctant to adopt the technology.
“We have some clients that really embrace technology and others that are more skeptical,” Cogbill said.
Despite these shortcomings, Rhodes said the need to incorporate telehealth will only grow, because younger workers, who will make up the future workforce, prefer it. “They’re big on self-service portals, online appointment scheduling and accessing mental health through apps,” she said.
“I think there are lessons we can learn from that group in terms of how we shape the future of telehealth and telemedicine.”
Cogbill foresees new technologies like wearables might increase telehealth use as well. A wearable device might be used to monitor an injury or a patient’s recovery remotely, she note
Lupinsky also sees a role for telehealth in reducing risk. He said CorVel is taking a proactive approach to reducing risk by identifying potentially costly claims.
For example, in the case of a patient using opioids, the CorVel team’s telehealth tech system might suggest to a provider they direct that patient to other methods of addressing pain.
“What we want to do is direct patients to other healthier alternatives,” he said.
“We can direct patients to a different mode of care such as cognitive behavior therapy or meditation.”
The pandemic shone a spotlight on telehealth, but the degree to which it will be accepted in workers’ compensation remains to be seen.
Lupinksy, for one, believes it will only grow. “The genie is out of the bottle,” he said. “I think it’s going to be tough to put it back in.” &
Annemarie Mannion is a freelance writer. She can be reached at [email protected].
CHARLESTON, S.C. (June 9, 2021) – A joint MUSC-Clemson panel of judges named the Parent-Child Interaction Therapy (PCIT) telehealth program as the first recipient of the Healthy Me – Healthy SC (HMHSC) grant. The HMHSC grant will provide a $50,000 award to support the Tele-PCIT program’s second year.
“We’re pleased to partner with and support Tele-PCIT, as it provides innovative therapeutic solutions to improve the quality of life for underserved South Carolina children and families,” explained David Sudduth, HMHSC executive director.
This was the inaugural year of the HMHSC grant, a funding opportunity designed to improve the implementation, reach and scaling potential of projects or programs that align with HMHSC’s mission to improve health care access and inequities in rural and underserved communities of South Carolina.
“The Tele-PCIT program application received high marks in each of our scoring categories and had a dual mental health and children’s health focus. We look forward to working with this program as it grows and helps additional families in need,” said Kapri Kreps Rhodes, HMHSC director.
All applications, she explained, needed to align with one of HMHSC’s four focus areas, which include women and children’s health, chronic disease/preventative health care, mental health and cancer. Applications were scored for their innovativeness, impact, scalability and sustainability.
The Tele-PCIT program
Disruptive behavior problems, such as oppositionality, aggression and hyperactivity/impulsivity, are present in 30% to 60% of children with autism spectrum disorder (ASD). PCIT is one of the most well-validated interventions for these types of behavior problems. Despite the initial promise of PCIT for children with ASD, challenges include attrition and limited accessibility.
Telehealth delivery has the potential to address barriers that affect treatment engagement, particularly for underserved populations. The Tele-PCIT program has spent the past year testing its feasibility and preliminary efficacy involving 20 children between the ages of 2 and 6 with ASD and disruptive behavior problems, with a considerable number of families coming from a low socioeconomic status or living in rural areas. The program provides parents with Bluetooth earpieces for the sessions and matches them with a PCIT therapist who then coaches them through 10 live PCIT sessions delivered to them via telehealth in their homes. The program has documented favorable outcomes regarding engagement and child behavior outcomes for families that have completed the program thus far. Its pilot will conclude this fall.
Rosmary Ros-DeMarize, assistant professor in the MUSC Division of Developmental-Behavioral Pediatrics and PI of the Tele-PCIT program, described the vision for the program. “While we know that PCIT has been well-established for young children with disruptive behavior via telehealth, the unique aspect of this program is expanding it to the ASD population, which is often in need of behavioral services. Our focus for the next year will be to reach families of young children with ASD from underserved communities to improve reach and accessibility of behavioral therapies.”
With the funding provided by the HMHSC grant, the Tele-PCIT program will expand its trial for an additional year to include a focus on an additional 20 children from underserved populations in an effort to increase reach and collect further preliminary data necessary for a randomized trial of PCIT within this population.
BAMBERG, SC—Palmetto Care Connections (PCC), a non-profit telehealth organization, recently received a $19,500 Rural Local Initiatives Support Corporation (LISC) grant and an additional $25,000 pledge from S.C. Department on Aging to implement a digital inclusion program for seniors in Allendale, Barnwell, Clarendon, Lower Richland and Williamsburg counties.
“COVID-19 has created an explosion in telehealth services and uncovered a tremendous need for internet access and digital literacy in rural areas,” said PCC Chief Executive Officer Kathy Schwarting. “As PCC surveyed rural health care providers, we confirmed that many of the seniors they serve have difficulty using and understanding technology, and many do not have internet access at home. The goal is to connect seniors not only to telehealth, but also to a variety of quality of life resources, such as special S.C. Arts Commission programs, to combat the social isolation that many seniors have faced during the pandemic.”
The Rural LISC grant and S.C. Department on Aging funding will help up to 100 seniors who live in rural communities, aged 65 and older, with digital literacy training, a free computing device and free cellular service for 12 months. PCC will work with local internet service providers to offer affordable internet packages for seniors and will help program participants apply for internet subsidies through the FCC Lifeline program. In addition, PCC will provide Digital Navigators to provide support and assistance throughout the pilot program.
“For more than 40 years, Rural LISC has proudly worked to connect communities with resources and access to opportunities that everyone deserves,” said Rural LISC Program Officer Christa Vinson. “PCC’s Digital Inclusion pilot program supports the mission of Rural LISC by providing the physical equipment and technical assistance that this segment of the population needs in order to access services and benefit from an increasingly technical society.”
“The South Carolina Department on Aging works with a network of regional and local organizations to develop and manage services that help seniors remain independent in their homes and in their communities. SCDOA is pleased to be a part of the PCC Digital Inclusion pilot program focusing on seniors in five of South Carlina’s rural counties,” said Kay Hightower, SCDOA Senior Consultant, Outreach and Partnership Building.
“It is our hope that this pilot program will be a model of one approach to closing the digital divide in South Carolina,” said Schwarting. “While PCC’s focus has traditionally been on serving rural health care providers with telehealth, broadband and technology resources, we have learned that patients need help in connecting to their health care providers. Residents of rural areas not only need internet access, they need access that is affordable and they need a device and knowledge to connect to resources for a better quality of life.”
“PCC is a member of the Digital Equity workgroup that is facilitated by the S.C. Office of Rural Health. Members include Rural LISC, S.C. Department on Aging, S.C. Arts Council, S.C. Telehealth Alliance, Revolution D and others who want to help close the digital divide in South Carolina. Through this committee we connected with Rural LISC and the S.C. Department on Aging to develop this pilot Digital Inclusion program for seniors in Allendale, Barnwell, Clarendon, Lower Richland and Williamsburg. We are grateful for their support and look forward to making a difference in the lives of some rural seniors,” said Schwarting.
Established in 2010, PCC is a non-profit organization that provides technology, broadband, and telehealth support services to health care providers in rural and underserved areas in S.C. PCC hosts the Annual Telehealth Summit of South Carolina presenting state and national best practices and trends, as well as providing networking connections for health care, information technology and broadband professionals. PCC co-chairs the South Carolina Telehealth Alliance, along with the Medical University of South Carolina, serving as an advocate for rural providers and partnering with organizations to improve health care access and delivery for all South Carolinians.
A bill to establish Medicare coverage for audio-only telehealth services is now in the House, setting the stage for a debate on whether the telephone is a good healthcare tool.
The debate over whether to allow Medicare coverage for audio-only telehealth services is now before Congress.
US Reps. Jason Smith (R-MO) and Josh Gottheimer (D-NJ) this week introduced the Permanency for Audio-Only Telehealth Act (HR 3447), which would establish coverage for healthcare providers who connect via phone or non-video telehealth platforms with patients who don’t have the resources to use video-based telehealth.
The bill would also remove geographic and originating site restrictions on Medicare coverage, allowing providers to collaborate with patients in their homes.
“The COVID-19 pandemic required the U.S. healthcare system to innovate and embrace every viable method of healthcare delivery. For patients in rural areas back home in Missouri, none have been more beneficial than the expansion of audio-only telehealth,” Smith said in a press release. “This method of healthcare delivery should serve as a bridge to provide better care and remain a permanent option for patients who will not gain access to broadband and technology overnight.”
Audio-only telehealth is a hot topic right now, with its supporters and opponents. The modality had been largely prohibited or strictly regulated prior to the pandemic, but has seen increased use thanks to emergency measures expanding access to and coverage of telehealth.
But those freedoms will end
Supporters not that many underserved and rural populations don’t have access to broadband resources needed to support audio-visual telemedicine technology, and they may not have the money to buy a smartphone, laptop or computer and Wi-Fi connectivity. In those cases a landline telephone may be the only good contact they have with care providers.
Organizations like the American Medical Association, Medical Group Management Association, Healthcare Leadership Council and Better Medicare Alliance have come out in favor of audio-only telehealth coverage, saying it improves access to care for a significant number of people who haven’t been able to access care.
“During the COVID-19 pandemic, audio-only visits have provided a lifeline to patients who are unable to attend visits in person or participate in telehealth visits due to lack of broadband access or necessary equipment to facilitate the visits,” Andres Gilberg, senior vice president of government affairs for the MGMA, said in the press release. “The need for these services will not disappear upon the conclusion of the COVID-19 public health emergency, but the ability to deliver them to Medicare beneficiaries will without congressional action. Patients should not be penalized for living far away from healthcare facilities or living in areas with inadequate internet access.”
Opponents argue the modality isn’t good enough to establish a doctor-patient relationship or to ensure privacy and security.
Most agree that if the modality is covered, the Centers for Medicare & Medicaid Services would need to develop guidelines as to how the platform can be used by providers, setting strict rules on what services can be provided.
If you’d talked to Brandon Welch in 2013, he probably wouldn’t have expected to be the CEO of a global leader in telemedicine.
Back then, Welch was a University of Utah doctoral student working on a hospital study to make prenatal checkups easier for pregnant women. Virtual visits made sense, but existing HIPAA-compliant platforms were complicated and expensive, so he built his own technology—just for the project.
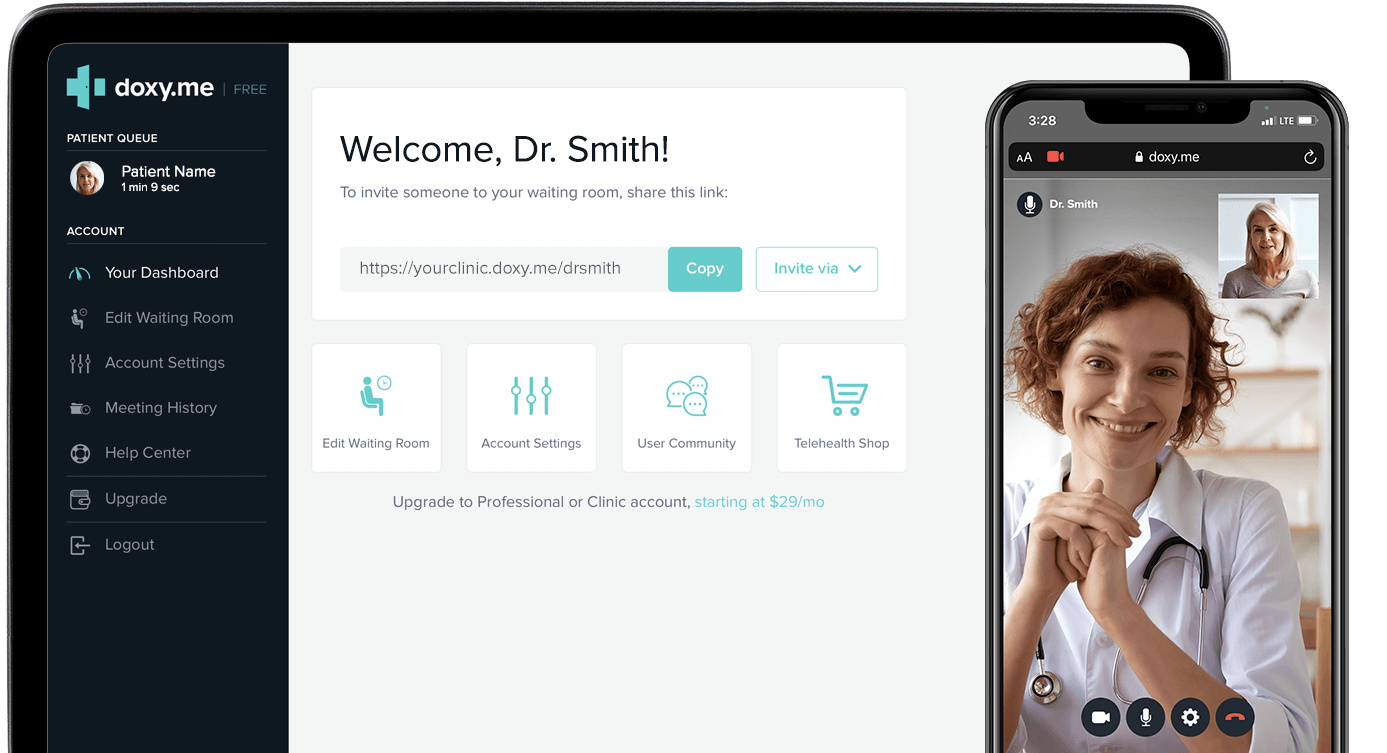
That led to use in a few more telehealth studies and to the launch of Doxy.me, a startup that offered a basic, secure platform for telehealth visits and a paid version with more features. The business grew through word of mouth, but it wasn’t intended to be a huge moneymaker. At one point, Welch took another job as a professor at the Medical University of South Carolina, while his co-founder Dylan Turner couch-surfed and worked in Salt Lake City coffee shops until the business paid his salary.
The Doxy.me platform, courtesy of Doxy,me
The pandemic created a rush for telehealth services
As you might have guessed, COVID-19 changed everything. Virtually overnight, doctors across the globe scrambled to figure out how to see patients remotely. Today, Doxy.me owns 30 percent of telehealth market share and has revenues in excess of $50 million. But this kind of fast growth was like walking a tightrope. “It was controlled chaos there,” says Welch. “And there were some white-knuckled moments.”
That was the case for many of Utah’s healthcare providers, its small number of telehealth platforms, and the state’s desperate patients. The number of telehealth medical claims in the state jumped 9,614 percent between December 2019 and December 2020, according to the nonprofit FAIR Health. Utahns mostly flocked to the web to see doctors and therapists for mental health, physical therapy, and specialists for respiratory, heart, and soft-tissue diseases.
“We’ve gone from telehealth being a novelty to being an accepted manner of care,” says Kerry Palakanis, director for ConnectCare, the telehealth arm of Intermountain Healthcare. Intermountain pioneered this telehealth platform in 2015 and saw its telemedicine appointments double early in the pandemic. “We were ready,” she says.
Welch, however, was caught off-guard by the sudden demand. Doxy.me had grown to 89,000 users in its first seven years. So on March 1, 2020, Welch was surprised when 100 providers signed up for the service— five times more than normal. He figured it was a fluke, but a friend in the United Kingdom warned Welch that this COVID thing might be a big deal. “We said, no that’s not going to be anything,” Welch recalls.
By the week’s end, Welch realized it was indeed a huge deal. By that point, 600 to 700 providers were signing up per day. The Doxy.me team jumped into action adding three new servers and automated bots to answer customers’ questions. They paused live onboarding sessions and created a YouTube video explaining the platform for new signups. “We used hundreds of support requests to refine the support and answer questions on our website,” Welch says.
Two weeks in, 5,000 people signed up in one day. The next day, 10,000 people signed up. The next day, 20,000 people. Two months into nationwide lockdown, Doxy.me ballooned to 600,000 providers and nearly 1 million sessions a day—up from the pre-pandemic base of 80,000 users and 12,000 daily sessions.
The fast growth blew Welch’s mind, and though it was a blessing, he knew if not handled properly it could crush the company. Doxy.me aggressively recruited at its Salt Lake and Charleston, S.C. offices, ramping up to 120 people from 10 employees the past year.
In those first few months of the pandemic, new recruits—some of these hires had been previously laid off from the restaurant business—holed up in Welch’s living room, building software, fixing bugs and answering support questions, working 12-hour shifts, stopping for dinner, then returning to work from 9 pm to 1 am.
Soon, Welch’s original pursuit of simplicity and easy access to telehealth became a magnet to providers everywhere. Other telehealth platforms might require weeks or months of onboarding before doctors or clinics could start seeing patients online, and video platforms like Zoom weren’t encrypted end-to-end. Doxy.me uses no computer in the middle to transfer information. The site doesn’t collect data and users are anonymous.
About half of Doxy.me’s users subscribed to the free version, which provided a basic room for a doctor and patient. The paid plans offered more perks, such as analytics, branding, billing, multiple rooms, and more. Suddenly, massive hospital networks with thousands of doctors wanted Doxy.me, and the team quickly created a new plan and features that could accommodate them, and also added seven more servers and built a chatbot to more quickly move people through virtual waiting rooms and into doctors’ “examination rooms.”
Brandon Welch, CEO, Doxy,me, courtesy of Doxy.me
The pandemic created demand for (and destigmatized) virtual therapy
While Welch scrambled to deliver on the hospitals and clinic front, entrepreneur Dallen Allred felt a similar surge in visits to his mental health startup Tava Health.
Allred and his wife Cami started Tava Health in 2019 to create a platform that employers could tap so workers could see a therapist or psychiatrist virtually. The couple recognized that Utah ranks among the worst in the US for access to mental health care. In some parts of Utah, patients must drive an hour just to get to a clinic, yet as many as 25.5 percent of the population struggles with mental illness.
Tava’s January 2020 launch proved to be perfect timing. Last summer, 40 percent of US adults reported struggling with mental health or substance abuse, according to the Centers for Disease Control. Virtual visits on Tava Health doubled during its first year of 2020. Yet before the pandemic, doctors and therapists resisted the idea of telehealth for fear of missing the subtle body language cues of patients when face-to-face.
That mindset immediately changed with COVID and has been reinforced ever since. According to Allred, mental health patient outcomes are actually better with telehealth. When a person can meet on their phone or laptop, it takes away the hassle and challenges of attending appointments. No-show rates dropped to five percent with virtual visits, compared to the average 30 percent, he says.
Buoyed by $3 million from investors, Tava Health plans to expand beyond its 100 paying employers this year—most of which are in Utah—and its 100 therapists licensed in 45 states.
Despite the new interest in virtual doctor visits, the sector still faces challenges ahead. The pandemic forced the federal government to fan the flames of telehealth by reducing telehealth regulations, which limited who could be seen, where, for what, and at what cost. Yet those waivers expire at the year’s end.
Now there’s talk of returning to many of the original restrictions on which kinds of visits are eligible and which kinds of patients can tune in remotely.
And insurers, too, may be more inclined to roll back some of their initial pandemic generosity, which included waiving copays and covering more types of virtual visits. In some cases, doctors were getting paid the same amount for virtual visits as they were for in-person visits—which had previously been a barrier to the adoption of telehealth. SelectHealth, Utah’s largest health plan, is already rethinking benefits, reimbursement rates, and planning for stricter criteria on what qualifies for telehealth.
When it comes to mental health, Utah still has regulatory barriers that will limit virtual appointments. Utah is among many states that still bar out-of-state therapists from providing mental health care to its citizens without going through a cumbersome and expensive licensure process. Yet the state lacks the therapists to meet demand. “It’s a stupid law, and it’s outdated,” says Allred.
Therapists also get paid 20 percent to 30 percent less for virtual visits than they do in-person visits. “There is very little that you can’t do well virtually when it comes to mental health,” Allred says. “You’re not listening to a heartbeat or lungs.”
The Tava Health platform, courtesy of Tava Health
Remote monitoring, virtual reality, and automated visits are coming
Though, the ability to listen to heartbeats and lungs from afar may come to a home near you soon. Intermountain’s ConnectCare is exploring new technologies for remote patient monitoring within its hospital network.
During the height of the pandemic, Intermountain gave newly diagnosed COVID patients mini COVID kits that included pulse oximeters and other technologies so doctors could remotely track their condition at home. The result: a 50 percent reduction in return ER visits. A $200 kit prevented what could have become a three-day, $3,000 hospital stay.
“I spend more time talking about remote monitoring than anything,” says Palakanis. She says the hospital system is exploring at least 20 other conditions where such technology could be useful—mostly in cardiac and lung disease.
Lots of data—heart rate, electrocardiograms, blood pressure, blood oxygen levels, kidney function, and more—can now be measured through remote wearables and used by doctors to manage care offsite. Recognition technologies, too, are being developed to pinpoint voice, emotion, gesture, posture—which could add to a doctor’s evaluation of a patient. And telemedicine could reduce provider workloads, cut the need for hospital or clinic space, and labor-intensive data entry. It could be helpful for post-surgical check-ins, prenatal visits, health education, and medication management.
These new technologies coincide with patients who have gotten very comfortable with virtual doctor visits, according to an October survey by healthcare IT firm DrFirst. Patients reported that during virtual doctor visits, they surfed the web, texted, played video games, sipped “quarantinis,” or drove in the car. Some didn’t even get dressed.
A little patient etiquette might be in order, but most people prefer the comfort of an online waiting room to one inside of a clinic. And that’s good news for startups like Doxy.me, because widespread adoption of the technology presents new opportunities to innovate.
With no outside investors calling the shots at Doxy.me, Welch says he feels more autonomous and free to innovate: “We’re going to create the future of what we think telemedicine should be.”
A Charleston resource center for people experiencing homelessness uses telehealth to provide medical care to one of the state’s most vulnerable populations.
More than 4,000 people in the state of South Carolina are experiencing homelessness. In the Charleston area, there are more than 400 homeless people: veterans, seniors, individuals and families.
“It’s really hard to get out of homelessness,” said Marie Elana Roland, CEO of The Navigation Center.
People typically live in “a crisis mode,” Roland said, because it is very difficult to escape homelessness. But The Navigation Center, located in downtown Charleston at 529 Meeting Street, provides food, housing support, employment services, hygiene care, and medical care through telehealth with doctors from the Medical University of South Carolina.
“Telehealth is an amazing technology for us,” Roland said. “They can just walk in and meet with MUSC and start their diagnosis. It’s a way for them to start getting healthy, so that they can make the right decisions and the right choices for their next steps.”
Layne Walker, a medical student at MUSC, and the first director of operations at The Navigation Center, said with the help of student volunteers, and telehealth technology, doctors are able to treat a variety of patient complaints all without leaving their office at MUSC.
Using digital equipment including a stethoscope and otoscope, the healthcare provider located at MUSC can hear and see throughout the exam.
“It’s as if the provider was in the room,” Walker said.
Cristin Swords Adams, DO, MPH, and Assistant Professor for the MUSC Department of Family Medicine, said providing care through telehealth allows her to bring medical care to patients who might not otherwise seek out care.
“This is an often stigmatized and marginalized population and often there’s a lot of distrust with the medical system,” Adams said. “We’re providing this care at a place where they’ve already developed relationships and they have trust.”
The agency hopes to get the OK at its June commission meeting to post a second Report and Order on the program, which aims to boost telehealth adoption by funding broadband expansion projects.
– The Federal Communication Commission is ready to move forward with its Connected Care Pilot Program, which aims to help providers expand their telehealth networks through better broadband connectivity.
The FCC is working on a Second Report and Order for the program, which launched in April 2020 and selected 14 applications for funding this January. More than 200 applications were received during the application window for the $100 million program.
According to a report issued by the FCC in advance of its June 17 commission meeting, the agency’s second report will help clarify how it identifies eligible services and provide more details to applicants on funding commitments, reimbursement and other aspects of the program. It would also give the green light to those selected in the first round to launch their three-year projects.
“The Commission received more than 200 Pilot Program applications from many health care providers whose patients lack Internet connections sufficient to transmit a video visit or receive health care through connected care and providers who indicate that their systems and bandwidth are inadequate to carry the new and significantly increased loads,” the FCC said in its report. “The projects we expect to announce in the future, as well as those announced in January 2, will directly benefit thousands of low-income patients and veterans facing a wide variety of health challenges, such as diabetes, hypertension, stroke recovery, opioid dependency, high-risk pregnancy, pediatric heart disease, mental health conditions, and cancer. Through these projects, we will develop a better understanding of how the Universal Service Fund (USF or Fund) can help support the adoption of connected care services among patients and their health care providers.”
The effort marks a slow-and-steady approach from the FCC for this program, and a departure from how the agency launched and managed its COVID-19 Telehealth Program. That program quickly blew through its $200 million budget in 2020, funding some 540 programs, but faced criticism from lawmakers and others over vague requirements and rules and a lack of transparency.
The second round of the COVID-19 Telehealth Program launched in April, with $250 million in new funding from the Consolidated Appropriations Act of 2021 and a pledge from the FCC to be more thorough in screening and approving applicants. The window for applications closed on May 6, and the FCC has yet to announce any award winners.
With the COVID-19 Telehealth Program and the Connected Care Pilot Program, the agency is focused on funding and supporting projects across the country that allow providers to improve the framework upon which connected care is delivered. Telehealth advocates say these programs are crucial to improving access to care for underserved and rural populations.
The health system invested heavily last year in telehealth and remote patient monitoring technologies to solve problems of the present and set itself up for the future.
First, staff recognized a high percentage of patients with diabetes or hypertension, or both, had unhealthy blood pressure (BP) and blood glucose (BG or A1c) metrics. High A1c levels indicate that a person might be at risk for diabetes.
Staff took a measure of all HopeHealth patients in December 2020 with these two problems:
A1c < or = 9, 70%
A1c > or = 9 / untested, 27.8%
BP <130/80, 30.7%
BP <140/90, 64.9%
“These simple metrics have a ripple effect in rural areas,” said Sean E. Whitfield, system integration analyst at HopeHealth. “Lack of care opportunities due to transportation, limited primary care locations and inadequate income opportunities can send many patients running to the emergency department.
“The need for early intervention through remote patient monitoring is key to saving patient lives and preventing unnecessary ED visits. For this problem, we adopted a remote patient monitoring solution from FORA Telehealth,” Whitfield continued.
Second, HopeHealth’s supply of telehealth hardware was out of date and lacked clinical peripherals. These constraints made it impossible to offer a comprehensive exam remotely.
“In 2019, we could only provide 156 telehealth visits for nutrition education and psychiatry,” Whitfield recalled. “As HopeHealth serves more than 50,000 patients, significant gaps in care in most centers were obvious. For this problem, we chose the vendor IronBow Technologies and specifically their Clinic Telehealth platform.
“Because we were painfully aware of the patient barriers that keep them out of care, each of these problems required funding,” he said. “When an FCC telehealth grant opportunity arose with a pandemic looming, it was high time to enhance and upgrade our services.”
PROPOSAL
For the health system’s RPM solution, the goal was to have patients achieve healthy BP and BG metrics over a set amount of time, using the devices to track progress. This program uses a 3G-enabled blood pressure and blood glucose monitor and a web-based electronic health record.
“Whether through partnerships with hospital systems, school systems and more unique monitoring programs, telehealth is here to stay, and we are looking toward the future.”
Sean E. Whitfield, HopeHealth
“Each patient would be requested to check their BP and BG multiple times a day, such as after a meal, when they wake up and before bed,” Whitfield said. “The RPM device then automatically submits this data to the EHR with a subsequent clinical pharmacist notification. Gathering this much data allows for early intervention of medication dosage, nutrition and lifestyle stressors.”
The bulk of HopeHealth’s investment in telehealth hardware came in the form of carts outfitted with the following equipment:
High-definition monitor.
Intuitive touch panel.
Point-tilt-zoom high-definition camera.
JedMed Horus with a general view lens and otoscope lens.
Omnisteth digital stethoscope.
The goal, which focused on the pandemic, was to alleviate the need to reschedule patients due to physician exposures to COVID-19. With physicians out of the office for up to three weeks, a logistical nightmare could develop without telehealth, Whitfield said.
“Each appointment reschedules a backlog of visits. Patients begin to run out of medications, have healthcare events, and add to already overwhelmed EDs,” he explained. “Procuring such specialized equipment also allows exponential advancement in our telehealth offerings. Now physicians can see and hear a patient with a telehealth presenter operating the examination peripherals from any of our centers.”
This qualification on its own allows the completion of comprehensive visits such as annual wellness check-ups for adults and children, he added.
MARKETPLACE
There are many vendors of telemedicine technology and services on the health IT market today. Healthcare IT News recently compiled a comprehensive list of these vendors with detailed descriptions. To read this special report, click here.
MEETING THE CHALLENGE
HopeHealth’s remote patient monitoring program started with a bang after acquiring 375 devices with $423,645 in FCC grant funding. The project manager issued instruments to the staff at most care locations and then distributed them to patients.
“The patients we provided devices to were mainly low-income patients who would never usually have access to technology or information like this,” Whitfield noted. “We encouraged each patient to check their metrics multiple times a day, and the clinical pharmacists export the reports to the eClinicalWorks EHR. Most of the results go to the individual patient’s primary care physician for final review.”
When the pharmacist reviews concerning data, they create an alert to have the patients’ clinical team intervene immediately. As this program stabilizes, staff can begin developing programmatic structures for the RPM groups. The plan will include RPM as a part of regular patient visits enhanced by nutrition and lifestyle education.
The carts began service immediately for physicians affected by COVID-19. Dr. Joseph D. Hoyle contracted COVID-19 in the fall of 2020 and had the following experience.
“When I had COVID, my employer offered me the option to continue working,” he explained. “My patients appreciated getting to keep their appointments and see the rest of their medical home team and me. My staff managed the peripherals while I directed the camera. Our shared documentation process did not change.
“I knew I could rely on the in-office vital sign measurement, office processes and nursing interventions,” he said. “The medical assistant and nurse prepare the patient chart with a pre-visit encounter and then usually dedicate a room for the patients to rotate with privacy for these visits.”
In primary care, a personal relationship is essential to disease management and anticipatory guidance, he added.
“Telehealth has maintained my relationship with patients during times of great need or isolation,” he noted. “Over the last year, the fear of COVID-19 has made many patients hesitant toward in-person visits. However, telehealth has allowed us to maintain or even improve patients’ health who have been able to engage with the technologies or access a telephone.
“The necessity of using telehealth over the past year keeps me optimistic for enriching my career,” he continued. “I look forward to blending intuitive telehealth to overcome barriers in healthcare, access and quality. Over time my team and I [have] become more confident in deciding which patients and complaints we can assess comprehensively using telehealth to diagnose certain conditions virtually.”
Dr. Hoyle’s experience is just one example of how HopeHealth used the telehealth carts during the pandemic. Many of the providers had this same experience when they either had a potential exposure or contracted COVID-19, Whitfield noted. A few specialists who were practitioners of telehealth got a nice upgrade from the outdated hardware in circulation, he added.
RESULTS
Preliminary results for the RPM program have seen some positives for the first group of patients. In these five months spanning December 2020 to April 2021, data indicates an average of positive outcomes for all 375 patients:
A1c < or = 9, December 64%, April 67%, +3%
A1c > or untested, December 35.1%, April 33%, -2.1%
BP < 130/80, December 30.5%, April 31.8%, +1.3%
BP < 140/90, December 65.2%, April 66.5%, +0.3%
“These patients decreased their A1c values and reduced their blood pressure,” Whitfield noted. “Only time will tell if this becomes a trend, but these outcomes are promising. Such data is validation that RPM can be a driver of patients controlling and maintaining their healthcare over time, and information is truly powerful.
“Implementation of the new telehealth carts allowed us to increase our patient visits throughout 2020,” he continued. “In 2019, with our existing hardware, we saw 156 patients via telehealth out of 218,050 total encounters. In 2020, we were able to see 21,013 patients virtually, out of 234,527, successfully. Of the 21,013 encounters, 20% [were] accounted for via telehealth carts, and direct-to-patient software accounted for 80%.”
Each maintained appointment stopped the ripple effect and allowed for prescription refills, labs, procedures and fewer chances of an ED visit.
“As a federally qualified health center, a large part of what we do is keep patients in care so EDs can focus on more significant issues like COVID-19 and non-preventable emergencies,” he added.
USING FCC AWARD FUNDS
In 2020, HopeHealth was awarded $423,645 by the FCC’s telehealth grant program for remote monitoring equipment and telemedicine carts stationed at 10 clinic sites throughout four counties, so providers exposed to COVID-19 who are required to self-isolate can continue seeing patients, and patients that are most vulnerable to the virus can be seen at home via telehealth remote monitoring devices for care coordination and medical tracking.
“The FCC telehealth award funds went to hardware purchases only,” Whitfield explained. “We bought 375 BP/BG monitors and 16 telehealth carts. We successfully expanded our RPM program from around 10 patients to 385 in a matter of months. We are now capable of comprehensive telehealth visits in all 14 care locations, up from only five in 2019.
“Not only are we able to see more patients, we feel that these resources provide a new point of access for them,” he added. “Our ability to provide patients with devices and accommodate travel restrictions levels the playing field for many individuals and overcomes barriers to care.”
For HopeHealth as a whole, the health system now is an accessible telehealth provider in South Carolina, he said.
“Many new conversations and potential partnerships are on the rise,” he concluded. “The hardware, staff training and awareness have us looking at new ways to deliver healthcare. Whether through partnerships with hospital systems, school systems and more unique monitoring programs, telehealth is here to stay, and we are looking toward the future.”
Palmetto Care Connections (PCC) is the telehealth network for South Carolina that offers telehealth support services to rural and underserved health care providers.